Findings
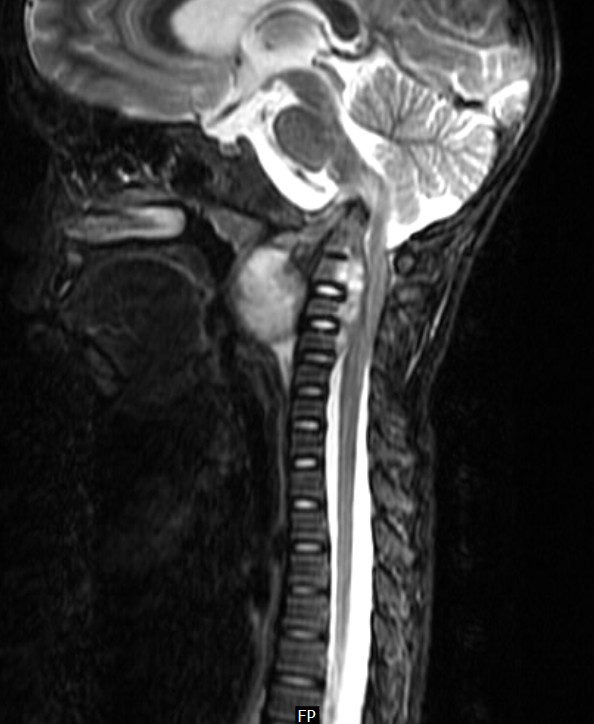
FindingsFigure 1: Sagittal T1 weighted image shows focal expansion of the cord substance in the region of the upper dorsal vertebrae (T3 and T4). The area is isointense to the cord.
Figure 2 and Figure 3: Sagittal T2 weighted and STIR images show a hyperintense lesion involving the dorsal spinal cord with edema, seen at its rostral and caudal ends. Incidentally seen is a hemangioma (Figure 1 and Figure 2) involving the T7 vertebral body.
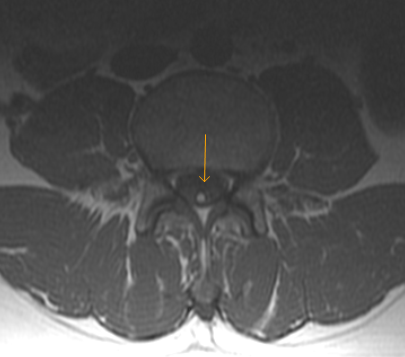
Figure 4 and Figure 5: Post contrast axial and sagittal T1 weighted images show almost homogeneous enhancement in the lesion. Incidentally seen are pleural effusion (Figure 5) and pulmonary metastasis (Figure 5).
Diagnosis: Intramedullary spinal cord metastases (ISCM) The most common neurological complications of breast cancer are brain metastases and spinal cord compression. In most instances spinal cord compression is caused by extra-dural soft tissue masses, however ISCM is a rare and a distinct diagnostic possibility.
ISCM is an unusual presentation of systemic malignancies. Close to 50% of all ISCMs arise from primary lung tumors, with small cell carcinoma being the most common. The remainder originate from primary cancers of the breast, colon, melanoma, lymphoma, and kidney. ISCMs are typically solitary and extend over a length of 2-3 vertebral segments.
The clinical manifestations of metastatic intramedullary spinal cord tumors are typically back pain, paresthesia, paraparesis, spasticity of the lower extremities, and autonomic dysfunction.
Magnetic resonance imaging is considered the gold standard for the diagnosis of tumors affecting the spinal cord. The typical ISCM seen on MRI is a small, isolated, oval-shaped lesion with or without slight deformation of the spinal cord profile. It is isointense on T1-weighted images with a nodular contrast enhancement and a pencil-shaped hyperintensity on T2-weighted sequences, most frequently extending proximal to the lesion. Cysts are rare, in contrast to primary intramedullary neoplasm.
External beam radiation with or without concomitant corticosteroids has been the most effective method of treating ISCM. In a small group of selected patients, surgical resection seems be a reasonable option, especially in cases presenting with previously undiagnosed or limited primary tumors and rapid neurologic deterioration. Also, when the primary tumor is well known to be radioresistant, as in the case of melanoma or renal cell carcinoma, surgical decompression or subtotal resection would be indicated.
Patients with ISCM have a very short life expectancy; their median survival is 3 to 4 months from the time of diagnosis. Those with breast cancer as the primary source of ISCM, tend to do better than other types of cancer; their median survival is 13 months.