Two papers from Radiology October 2010 are featured here to update the readers of the exciting updates in the field of medical imaging.
Few days back we had post coiling patient who post the procedure deteriorated. Plain CT scan showed increased sulcal density in the area, which could have been persisitent post angiographic contrast versus rebleed. Going through the article "Evaluation of Dual-Energy CT for Differentiating Intracerebral Hemorrhage from Iodinated Contrast Material Staining- October 2010 Radiology, 257,205-211." , possibly dual energy CT is the answer
Right Coronary MR Angiography at 7 T: A Direct Quantitative and Qualitative Comparison with 3 T in Young Healthy Volunteers- October 2010 Radiology, 257,254-259 has found improvement in evaluation of right coronary artery using 7Tesla MRI versus 3T.
Sunday, October 31, 2010
Acute cerebellitis-MRI
Acute cerebellitis is one of the main causes of cerebellar dysfunction in children, and may be infectious, post-infectious or post-vaccination. Its aetiology is usually viral and a large number of viruses have been implicated (varicella-zoster, measles, mumps, coxsackie, Epstein-Barr, rubeola, pertussis and diphtheria, among others), although in most cases a definite aetiology remains undetermined . The cerebrospinal fluid examination may be normal or reveal pleocytosis, and the diagnosis is based mainly on clinical criteria . The disease is usually benign and self-limiting, its prognosis is habitually good, and recovery with a few or no sequelae is the usual outcome
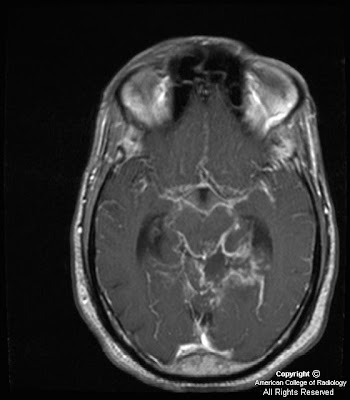
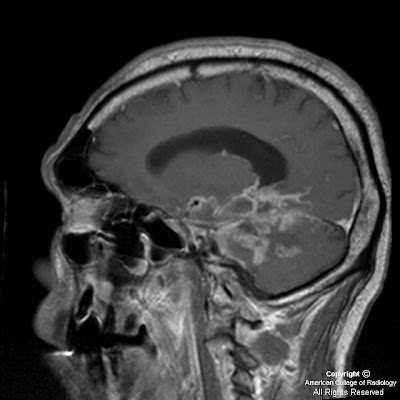
IMAGING- It is usually bilateral,symetrical and MRI is the investigation of choice It displays predominantly graymatter and cortical signal abnormality with white matter involvement, which when it occurs is patchy and variable ,compressing the 4 th ventricle leading to obstructive proximal hydrocehalus. It is usually is low on T1 and bright on T2 and FLAIR with NO restricted diffusion(diff from acute infarction). Restricted diffusion is more common in bacterial and anerobic cerebellitis , though it can be seen in viral eiology Contrast enhancement is typically pial and along the sulcal spaces. MRS shows necrosis ,as lactate/ lipid in occassional cases
Differential diagnosis-- include acute intoxication by drugs, alcohol, tumours and demyelination (predominantly white matter involved). Lead poisoning could simulate this and so does Lhermitte-duclos (LDD)which could be differentiated by the presence of contrast enhancement and full recovery in cases of viral cerebellitis . If any surgical intervention is planned, in any caae resembling this disease ,it is worth repeating MRI after few weeks to see progress as viral cerebellitis will invariably improve.
Case by Dr MGK Murthy, Sr Consultant Radiologist.




IMAGING- It is usually bilateral,symetrical and MRI is the investigation of choice It displays predominantly graymatter and cortical signal abnormality with white matter involvement, which when it occurs is patchy and variable ,compressing the 4 th ventricle leading to obstructive proximal hydrocehalus. It is usually is low on T1 and bright on T2 and FLAIR with NO restricted diffusion(diff from acute infarction). Restricted diffusion is more common in bacterial and anerobic cerebellitis , though it can be seen in viral eiology Contrast enhancement is typically pial and along the sulcal spaces. MRS shows necrosis ,as lactate/ lipid in occassional cases
Differential diagnosis-- include acute intoxication by drugs, alcohol, tumours and demyelination (predominantly white matter involved). Lead poisoning could simulate this and so does Lhermitte-duclos (LDD)which could be differentiated by the presence of contrast enhancement and full recovery in cases of viral cerebellitis . If any surgical intervention is planned, in any caae resembling this disease ,it is worth repeating MRI after few weeks to see progress as viral cerebellitis will invariably improve.
Case by Dr MGK Murthy, Sr Consultant Radiologist.




Friday, October 29, 2010
Pott's Puffy Tumor








Findings
Figure 1: The image shows a large collection anterior to the frontal bone and a large epidural abscess with peripheral enhancement.
Figure 2: Erosion of the frontal bone. Sinus tract of the bone into the large anterior collection.
Figure 3: Large collection anterior to the frontal bone.
Figure 4: Large epidural abscess.
Figure 5: Large epidural abscess with peripheral enhancement.
Figure 6: Large collection anterior to the frontal bone. Large epidural abscess. Normal bone marrow signal. Abnormal bone marrow signal in the frontal bone.
Figure 7: Large collection anterior to the frontal bone with peripheral enhancement. Large epidural abscess with peripheral enhancement.
Figure 8: Abnormal bone marrow signal in the frontal bone. There is a lack of enhancement of the frontal bone. The abnormal dark bone marrow signal on T1 images and lack of enhancement on T1 post gad fat sat is consistent with dead necrotic bone from severe osteomyelitis.
Diagnosis: Pott's Puffy Tumor
Pott’s puffy tumor is a subperiosteal abscess of the frontal bone that appears as a localized swelling of the forehead associated with frontal osteomyelitis. Pott’s puffy tumor is a complication of frontal sinusitis or trauma, which is predominatly seen in the adolescent age group. However, there are a few case reports in adults. Pott’s puffy tumor is a rare complication of frontal sinusitis in the post antibiotic era but can be seen in patients with undiagnosed or partially treated sinusitis. Patients will typically present with frontal scalp swelling, headache, fever, nasal drainage, and frontal sinus tenderness. Ocassionally, Pott’s puffy tumor can mimic findings of preseptal or orbital cellulitis. In severe cases, there will be neurologic decompensation. Varying degrees of hemiparesis, obtundation, papillary dilatation or aphasia have been described in case reports.
Imaging is necessary to exclude intracranial complications such as epidural abscess. Pott’s puffy tumor can also be associated with dural sinus thrombosis, meningitis, subdural empyema, epidural abscess, brain abscess, and rarely seizure. Intracranial infection is caused by posterior extension from the frontal sinus while preseptal and orbital cellulitis is caused by downward spread from the frontal sinus to the orbit. Younger children who do not have pneumatized frontal sinuses, are more likely to have ethmoid sinusitis. Orbital cellulitis is a more common complication in patients with ethmoid sinusitis.
Patients must be treated with a combination of surgery and long-term antibiotic therapy.
Thursday, October 28, 2010
Atypical Sites Of Metastasis-Two Cases
These are two atypical sites of secondaries in recent past in my practise, which we are sharing in our site.
The metastatic lesions of pancreas are extremely rare. Tumors metastasizing to the pancreas include lung carcinoma, gastrointestinal tract carcinoma, breast carcinoma, renal carcinoma, melanoma, lymphoma, and (osteo)sarcoma. This is a 15 year old girl known case of osteosarcoma, with suspected pancreatic secondaries.
Another atypical case, is a 67 year old male with past nephrectomy for hypernephroma and had shoulder pain. MRI done revealed altered marrow signal intensity involving the glenoid process of scapula along with involvement of the coracoid process. There is evidence of associated osseous destruction and soft tissue component. Similar cases of glenoid secondaries has been reported previously in the literature especially with hypernephroma. Reference-Daluga D, Quast M, Bach Bernard, Gilelis S. Shoulder neoplasms mimicking rotator cuff tears. Orthopaedics 1990 July; 13:765-767.


Monday, October 25, 2010
Brodie's Abscess-CT
Classical radiological features are oval elliptical or serpiginous radiolucency usually around 1cm surrounded by a reactive sclerosis, granulation tissue, and a Nidus often less than 1cm. The margins often appear scalloped on radiograph. Brodie's abscess is best visualized using CT scan. Tunnelling is a classical sign of brodie's abscess.




Infected 4th Branchial apparatus cyst




Findings
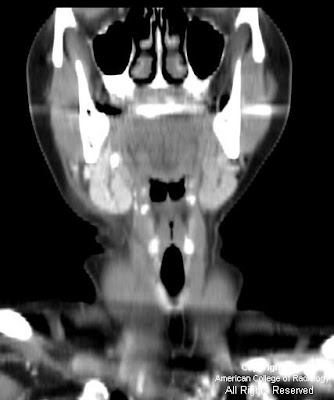
Figure 1: Neck CT, contrast enhanced, at level of pyriform sinus. The left pyriform sinus is effaced by an inflammatory mass.
Figure 2: Neck CT, contrast enhanced, at level of subglottic trachea. The image demonstrates continuation of the large inflammatory mass with small areas of necrosis or abscesses. Note displacement of the trachea to the right and lateral displacement of the carotid sheath vessels. Reactive lymphadenopathy is present in the internal jugular chain.
Figure 3: Neck CT, contrast enhanced, at level of the thyroid gland. The image shows a mixed attenuation mass in the enlarged left lobe of the thyroid. This mass arises from extention of the extrinsic anterior and lateral inflammatory mass with phlegmon and abscesses from an infected 4th branchial apparatus cyst.
Figure 4: Neck CT coronal reformation, contrast enhanced. There is extensive phlegmon with multiloculated abscesses, extending from the left lower pharyngeal wall into the left lobe of the thyroid gland. Reactive lymphadenopathy in the left internal jugular lymph node chain is present.
Diagnosis: Infected 4th Branchial apparatus cyst
The main differential diagnostic considerations for a cystic neck mass in children include suppurative lymph nodes, abscess, thyroglossal duct cyst, lymphatic malformation, ranula, and branchial apparatus cyst. A branchial apparatus cyst (BAC) results from maldevelopment of an embryonic branchial apparatus (branchial cleft, arch, and pouch). Embryologically, 6 mesodermal branchial arches, separated by 5 external ectodermal branchial grooves (clefts) and 5 internal endodermal branchial pouches are present bilaterally. The majority of branchial apparatus anomalies are cysts that can arise from a remnant of a groove, arch, or pouch. A 2nd BAC is the most common and accounts for >90% all branchial cleft anomalies discovered in teens and adults. It represents 66%-75% of these anomalies discovered in children.
A 1st BAC is typically found as a cystic mass around the pinna or extending from external auditory canal (EAC) to the angle of the mandible. It can communicate with the external auditory canal. The 2nd BAC is typically found at or immediately caudal to the angle of the mandible, lateral to the carotid space and anteromedial to the sternocleidomastoid muscle. An associated fistulous track may extend from the cyst between the external & internal carotid arteries to the palatine tonsil. The cyst can extend to the carotid bifurcation, producing a beaked configuration, which has been called the "notch sign" and which is considered pathognomonic for a 2nd BAC. The 3rd BAC is typically found in the posterior cervical space behind the carotid sheath in the upper neck and along the anterior border of sternocleidomastoid muscle in the lower neck.
A 4th BAC is rare and seen more often in female infants. It can occur anywhere from the apex of pyriform sinus to the ipsilateral thyroid lobe. Involvement with the thyroid can be understood by noting that the thyroid gland arises from the 4th branchial arch. The most typical imaging finding of a non-infected 4th BAC is a unilocular thin-walled cyst found adjacent to or within the superior lateral aspect of the left thyroid lobe. Ninety-four percent of BACs involve the left side of the neck. These cysts normally show minimal or no peripheral contrast enhancement and no calcification. When infected, a thickened cyst wall is seen and often enhances with intravenous contrast media. Infected cysts often develop higher attenuation than noninfected cysts on CT images. Associated thyroiditis/thyroid abscess is not uncommon. An esophagram may demonstrate fistulous communication between the pyriform sinus and a 4th BAC, providing a pathway for spread of infection. Surgical resection of the cyst and its associated sinus or fistulous tract is necessary for complete cure. Medically treated or incompletely resected cysts/tracts are prone to recur.
Friday, October 22, 2010
Double stent assisted coiling of a complex basilar top aneurysm-Video
Rupture of brain aneurysm (A balloon like swelling over a blood vessel) results in brain hemorrhage (Subarachnoid Hemorrhage- SAH). Patients present to the emergency with a complaints of "worst headache of their life." Treating the aneurysm in a patient of SAH if of paramount importance, as aneurysms are know to have very high risk of re-bleed leading to death of patients
Please click the link below to see Double stent assisted coiling of a complex basilar top aneurysm with both PCAs and both SCAs coming out of the aneurysm.
http://www.youtube.com/watch?v=0HBp1wOlpxY

Case submitted by- Dr. Sibasankar Dalai, MD, FACP
Fellow, Australasian College of Phlebology,
Member, American College of Phlebology,
Please click the link below to see Double stent assisted coiling of a complex basilar top aneurysm with both PCAs and both SCAs coming out of the aneurysm.
http://www.youtube.com/watch?v=0HBp1wOlpxY

Case submitted by- Dr. Sibasankar Dalai, MD, FACP
Fellow, Australasian College of Phlebology,
Member, American College of Phlebology,
Adenoid cystic carcinoma with perineural spread of tumor







Findings
There is a large mass centered on the left greater sphenoid wing, extending into the left sphenoid sinus and left pterygopalatine fossa. It also extends into the left middle cranial fossa, left cavernous sinus, and left Meckel's cave. The tumor has involved V3, and foramen ovale is markedly widened on the left. There tumor has extended along the GSPN to the geniculate ganglion, and from there it has involved the tympanic and intracanalicular segments of the 7th nerve. The mass is isointense to brain on T1-weighted images and hypo- to isointense on T2-weighted images, consistent with hypercellularity. There is moderate enhancement of the mass. No macroscopic flow voids are seen to suggest a highly vascular lesion.
Figure 1: A mass lesion involving the skull base and pterygopalatine fossa on the left is shown on this axial FIESTA image. Abnormal soft tissue is seen in the left IAC as compared to fluid in the right IAC. The normal right greater wing of the sphenoid bone is shown. On the left, the greater wing of the sphenoid has been destroyed by the mass.
Figure 2: The soft tissue intensity skull base mass is again shown on the left. Infiltration of fat in the L pterygopalatine fossa is present, as compared with normal bright fatty signal in the R PPF. Asymmetrical signal is again seen in the left vs right IAC.
Figure 3: Following injection of gadolinium, moderate homogeneous enhancement of the mass lesion is shown. Also appreciated is extension into the L sphenoid sinus and displacement of the left cavernous segment of the L internal carotid artery. Meckel’s cave on the L is obliterated. Abnormal enhancement in the left IAC and abnormal thickening and enhancement of the tympanic segment of the facial nerve are also shown. Subtle linear enhancement extends posteriorly from the dominant mass along the greater superficial petrosal nerve on the left.
Figure 4: A more superior post-gadolinium image more discretely defines enhancement and enlargement of V3 on the left, posterior to the main bulk of the tumor mass. Tumor is again seen to extend posteriorly along the GSPN to the geniculate ganglion.
Figure 5: Tumor is seen to involve and expand Meckel’s cave on the left, replacing the normal CSF signal with intermediate signal intensity of a highly cellular tumor. The unaffected Meckel’s cave on the right, filled with CSF, is shown for comparison. The tumor is confined to Meckel’s cave on this image and has not extended through the dura to involve the adjacent temporal lobe.
Figure 6: A more anterior coronal T2-weighted image shows extension of the tumor into the cavernous sinus on the left, adjacent to the flow void of the internal carotid artery. Marked thickening of the third or mandibular division of the trigeminal nerve is shown on the left. The mass has markedly expanded foramen ovale on the left. This image also demonstrates atrophy and mild T2 hyperintensity of the muscles of mastication on the left, due to V3 dysfunction and resultant subacute to chronic denervation change. The masticator muscles on the right have normal bulk.
Figure 7: The enhancing tumor mass involving Meckel’s cave and the cavernous sinus on the left is again shown. This image better demonstrates the unaffected foramen ovale on the right. Also demonstrated on this image is volume loss and diffuse mild enhancement of the left temporalis muscle as compared to the right, consistent with denervation change as previously discussed). Signal drop-off due to dental hardware and inhomogeneity of the magnetic field has resulted in artifact and poor fat suppression in the right masticator space.
Diagnosis: Adenoid cystic carcinoma with perineural spread of tumor
Adenoid cystic carcinomas have a high propensity for perineural invasion and extension.
The facial and trigeminal nerves are the cranial nerves most commonly involved by perineural spread of tumor.
The facial nerve may be invaded directly by tumors of the parotid gland, or the tumor may involve the trigeminal nerve and then extend along the greater superficial petrosal nerve to reach the facial nerve.
A second “five-to-seven” connection is the auriculotemporal nerve, which also provides an important route for perineural spread of tumor.
The proximal greater superficial petrosal nerve, geniculate ganglion, and tympanic segment of the facial nerve often show normal mild enhancement due to investment by a rich vascular plexus in these regions.
Characteristics of perineural extension of tumor include abnormal enhancement and enlargement of nerves, replacement of fat in neural foramina, and widening of neural foramina. Denervation changes in innervated muscles may also be observed.
Adenoid cystic carcinoma (ACC) is the second most common malignant salivary gland tumor after mucoepidermoid carcinoma. It can arise from either the major or minor salivary glands. It is the most common malignancy of the submandibular and sublingual glands. It most commonly presents as a painless enlarging mass, though the initial presentation may be due to perineural extension of tumor (pain or paresthesia, for example) if the tumor is in a deep location. ACC is associated with a high risk of distant metastases (most commonly to the lung), and these can occur 10-20 years after initial diagnosis and treatment of the primary lesion. ACC may spread through local or direct extension of the tumor, hematogenous and lymphatic dissemination, and perineural extension.
ACC has a high propensity for perineural invasion and extension. SCCs also have a high tendency to spread perineurally, and because they are the most common head and neck cancer, one will likely encounter more cases of perineural tumor spread from SCC than from ACC in practice. Other cancers of the head and neck, including melanomas, basal cell carcinomas, and mucoepidermoid carcinomas also extend perineurally, but less commonly. Branches of the facial and trigeminal nerves are most commonly involved as they innervate the cutaneous and mucosal surfaces of the head and neck, where most tumors arise, as well as the salivary glands. The facial nerve can be invaded directly when ACC occurs in the parotid gland, or the tumor may involve the trigeminal nerve and then extend along the greater superficial petrosal nerve to reach the facial nerve. An alternate route for cranial nerve 5 to cranial nerve 7 spread (or vice versa) is the auriculotemporal nerve, which is located posterior to the neck of the mandible.
The greater superficial petrosal nerve emerges from the geniculate ganglion of cranial nerve VII carrying sensory (from the soft palate mucosa) and parasympathetic fibers. It courses anteromedially through the temporal bone and emerges through the facial hiatus. It then travels underneath Meckel’s cave and combines with the deep petrosal nerve (carrying sympathetic fibers) to form the vidian nerve. The vidian nerve travels anteriorly to the pterygopalatine ganglion, where the parasympathetic fibers synapse before being distributed to the lacrimal gland and mucosal glands of the nasal and oral cavities. This nerve pathway is vulnerable to tumor infiltration and is a common pathway for perineural extension of tumor.
Portions of the facial nerve that are invested with a rich vascular plexus may normally enhance on MRI. These normally enhancing regions are the proximal greater superficial petrosal nerve, geniculate ganglion, and tympanic segment of the facial nerve; the labyrinthine and descending mastoid segments of the facial nerve may also show mild enhancement under normal circumstances. The more distal and anterior portions of the greater superficial petrosal nerve, however, are not invested by a vascular plexus and should not enhance with contrast on MRI. Similarly, the facial nerve in the IAC does not demonstrate any enhancement under normal conditions at 1.5T. Characteristics of perineural spread to the facial nerve include thickening and abnormally intense enhancement of nerve segments, as well as replacement of fat in neural foramina by tumor. Denervation changes in the muscles of facial expression may be observed, but these are often extremely subtle due the small size of the affected muscles. Due to ACC’s high propensity for perineural spread and high tendency to recur, it is important to regularly assess for perineural extension of these tumors when MR images are being interpreted.
Wednesday, October 20, 2010
Sialadenitis with an obstructing sialolith in the right submandibular gland duct

Findings
Coronal and axial post contrast CT images show a swollen right submandibular gland with dilatation of the intraglandular ducts and an obstructing stone.
Diagnosis: Sialadenitis with an obstructing sialolith in the right submandibular gland duct
The most common cause of sialadenitis of the SMG is an obstructing calculus with subsequent suppurative sialadenitis. Less common causes are suppurative sialadenitis leading to duct stenosis and chronic sialadenitis. Rare etiologies include include Sjogren syndrome, AIDS and bacterial/viral infection.
SMG accounts for 10% of sialadenitis of all major salivary glands. Other diagnostic considerations in SM space include reactive submandibular lymph node, mandibular osteomyelitis, benign mixed tumor, submandibular carcinoma and metastases.
Calculi are more common in the SMG duct. Compared to the parotid gland, the saliva in the SMG is thicker, much more mucinous and more alkaline. The SMG duct courses superiorly which makes it more prone to stasis. SMG duct is larger in diameter.
When sialadenitis is present therapy may depend on stone location. If the stone is in the anterior portion of the duct, the stone can be removed and gland salvaged. If stone is in the posterior duct, the duct and gland will likely be removed with the stone.
Pulmonary Fibrosis- CXR
76 yr old compalints of shortness of breath with history of COPD with decreased oxygen saturation with no definite occupational history relating to toxins/pollutants. There is extensive, ill defined reticular hard shadowing in all zones with suggestion of Rt CP angle blunting and rt diaphragmatic, possible calcium with no significant Rt ventricular enlargement on this film.
Best described as Dirty lung fields.
Teaching points
-Hard reticular shadows with some subpleural nodules with at places loss of tissue interfaces
-Rt pleural thickening along with plaque diaphragmatic region
-Questionable mediastinal adenopathy
-Few areas of focal hyper inflation
-Heart not conformity to COPD with pulmonary conus not full
Xray diagnosis could suggest Pulmonary fibrosis - needs compariosn with old Xrays/ HRCT evaluation
Pulmonary fibrosis
Definition: literally scarring andreplacemnt of lung tisue with fibrous tisue
Classification: at the most confusing and rapidly changing as the etiology and types are broad progresses rapidly after 40s and 50 s, presents with shortness of breath and dry cough, typically misdiagnosed initially in view of clinical mimic to infection/embolism/COPD/ heart failure /Asthma etc. Xray chest could be normal adding to the misdiagnosis
Restrictive lung disease suggested by maintained FEV1/Fvital capacity , though the latter is decreased depending on the etiology radiolgical features vary idiopathic may show usual interstitial patern(UIP)

More on this will be presented with HRCT picture -look out for it.
Tuesday, October 19, 2010
Adenosquamous Carcinoma Lung-CT
50 year male with cough and CT showed a large well defined regular, heterogeneously enhancing , peripheral , broadbased , noncalcifying, nonnecrotised SOL with no defintie bronchus cutoff. The medial and proximal lung of upper lobe displays airbronchogram. Mediastinal lymphadenopathy of moderate size is suggested in paratracheal and precarinal region with possible involvement of ipsilateral hilum. Ribcage, pleuralmargin, soft tissues, rest of the lung fields and adrenal glands are normal along with supraclavicular regions. CT value suggests solid lesion consistent with mass lesion
CT guide FNAC suggested adenosquamous carcinoma
AdenoSquamous carcinoma is unusual and rare pulmonary malignancy with two distinct cell types. Constitutes only 0.4 to 4% of all pulmonary malignancies.
Etiology: can arise from damaged parenchyma posibly from pneumoconiosis, and radiaiton fibrosis
Histology was defined by WHO in 1982 , modified by japanese lung society recently with suggestion of atleast 10% of microscopic appearance from both adeno and squmous components This can arise by collison of two adjacent tumours and yet distinct tumours , or as some consider as high grade mucoepidermoid ca with high squamous content or adenoca with squamous metaplasia
Studies-Mass Gen Hosp reports them to be peripheral in 83%, right lung involv in 63%,size varying from 7 to 65 mm with presence of cavitation in only 14%. It has been recently reported in chest journal presenting as multiple cavitating nodules mimicking infections . Prognosis is generaly considered poor with nagasaka et al reporting 6.2%survival at 5 yrs compared to appx 42% each for adeno and squamous varieties amongst review involving 1400 cases.
Case Submitted by – Dr Sudheer , Dr Krishnamohan and Dr MGK Murthy



Monday, October 18, 2010
Basilar meningitis of unknown etiology



Findings
Figure 1,Figure 2, Figure 3, Figure 4: Axial and sagittal T1 weighted images postcontrast demonstrate thick and nodular predominantly basilar meningeal enhancement which on sagittal images encases the middle cerebral arteries. Cerebellar parenchymal enhancement (Figure 4) secondary to late subacute infarction and infectious/inflammatory exudates.
Figure 5: Axial T2 weighted image demonstrates slight increased size of lateral ventricles with more prominent frontal horn lateral ventricles and bilateral lateral ventricle atria in a 2 week follow-up study (initial study slightly motion degraded.)
Diagnosis: Basilar meningitis of unknown etiology (presumed MDR-Tuberculosis)
This young patient with immunocompromise and altered mental status presented initially with left posterior circulation infarctions of unclear etiology. In a young patient with posterior circulation infarctions, acute vertebral artery dissection/ injury in the setting of trauma or spontaneous etiology should be considered. However, when given a history of immunocompromise and HIV, other differential diagnostic considerations such as infectious (Tuberculous, fungal, or pyogenic), inflammatory (Neurosarcoidosis), vascular (infectious vasculitis from Neurosyphilis or HIV), or neoplastic (lymphoma, leukemia, leptomeningeal carcinomatosis) etiologies should all be taken into account. To date, laboratory and CSF values for this patient continue to be non-diagnostic as to the source of this patient's basilar meningitis/vasculitis. The top consideration after discussing with the neurology team is Multi-drug resistant tuberculosis (MDR-TB) due to unimpressive response to conventional treatment regimens and inconclusive microbiological testing.
Tuberculous CNS infections are mostly caused by M. tuberculosis; atypical organisms are rare except in immunosuppressed patients. 30% of patients are HIV positive (particularly IV drug users.) Due to hematogenous dissemination, lesions usually occur at the gray-white junctions of cerebral hemispheres, basal ganglia, or cerebellum (especially in children). Hematogenous dissemination is from a systemic source, most commonly the lung, but also possibly the GU system or GI tract.
Most common manifestations of CNS Tuberculosis are meningitis, seen predominantly in the basilar cisterns, and hydrocephalus. Acutely, cerebritis can be seen, which then can progress to ring-enhancing tuberculoma lesions. Tuberculosis can also result in vasculitis and cerebral infarctions. The thick and nodular basilar meningeal enhancement in association with hydrocephalus and left posterior circulation multifocal infarctions in our patient can all be seen in tuberculosis.
Leptomeningeal sarcoidosis must be distinguished clinically from carcinomatous, lymphomatous/leukemic, and infectious meningitis. Dramatic response can be seen in some cases with steroid therapy. Sarcoid has replaced syphilis as the great mimicker. Neurosyphilis can cause arteritis of intracranial and extracranial large and medium sized arteries
Air Mensicus Sign in Hydatid Disease
In chest roentgenograms, the pulmonary meniscus sign is a crescent-shaped inclusion of air surrounded by consolidated lung tissue. The common cause is aspergilloma. A hydatid cyst is, however, the most common cause in endemic areas. Cyst growth produces erosions in the bronchioles that are included in the pericyst, and, as a result, air is introduced between the pericyst and exocyst, producing the crescent or meniscus sign. Air penetrating the interior of the cyst may outline the inner surface of the exocyst, producing parallel arches of air that are referred to as Cumbo's sign with an “onion peel” appearance.




Saturday, October 16, 2010
Carpal Tunnel Syndrome-MRI
62 yr old house wife has clinical symptom of falling objects from the wrist with electrophysiological data of median nerve compression has reported for MRI. MR axial images show degenerative changes in the wrist in general , median nerve appears compromised within the canal with ratio of width to height nearly 2.0 and bowing of retinaculum with height of the canal at upper border of normal(1cm)
Radiological points of interest
Definition: fibroossoeus passage from palmar side connecting distal forearm to midlepalmar region
Contents: Total 9 tendons
Flexor digitorium profoundus 4
Flexor digitorium superficialis 4
Flexor pollicis longus 1
Nerve 1 = median nerve passes between FDP and FDS
FDP and FDS are enclosed in ulnar sheath and FPL is enclosed in radial sheath. From hook of hammate to trapezium tubercle extends the flexor retinaculum and the height of the canal is usually 10mm. Median nerve can show flattening (rep by increased width/ height ratio), ill defintion, more signal intensity on fat suppression (compared to hypothenar muscels ), and enhancement on CEMR, age related quantitative studies showed volume increase with age, anatomical variations and dynamics of flexion/ extension of wrist affect the relative space for median nerve. Newer developments include calculation of age related volume measurements, dynamic study of the joints, and posibly MR neurography.
Case by Dr MGK Murthy, Sr Consultant Radiologist
Prime Telerad Providers (P) Ltd.



Marjolin Ulcer
Dr. Jean Nicolas Marjolin first described the occurrence of ulcerating lesions within scar tissue in 1828. Marjolin’s ulcer is the term given to these aggressive epidermoid tumors that arise from areas of chronic injury, with burn wounds being a common site.




Subscribe to:
Posts (Atom)