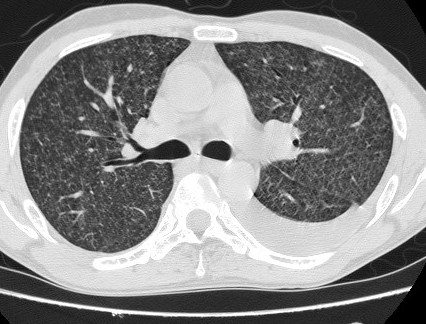
Additional clinical history: Acute leukemia.
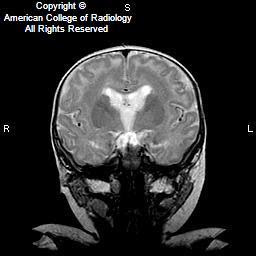
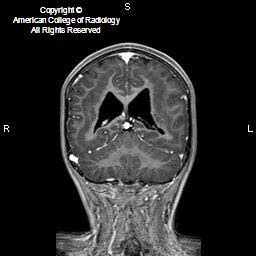
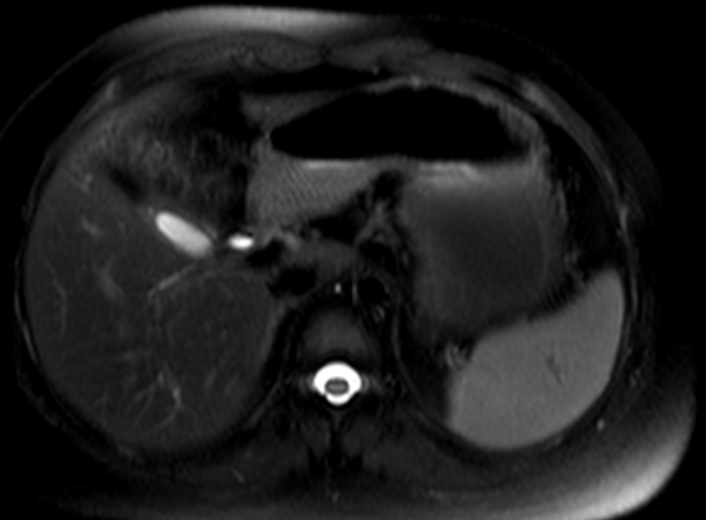
FindingsLarge anterior epidural mass extending from posterior clinoid to the cervicothoracic junction measuring approx. 6x3x1.5 cm with mass effect on the anterior pons, medulla, and upper cervical cord. No post-contrast imaging obtained.
Differential diagnosis: Epidural mass
- Metastatic disease
- Lymphoma
- Leukemia/chloroma
- Chordoma
- Osteomyelitis/epidural abscess
- Epidural hematoma
- Primary tumor such as neurofibroma/schwannoma
Diagnosis: Chloroma of epidural spaceKey points AKA granulocytic sarcoma, extramedullary myeloblastoma.
Most commonly occurs in the setting of AML.
Can also occur in setting of chronic myelogenous leukemia and other myeloproliferative disorders.
These tumors can involve any part of the body, either concurrently or sequentially.
Imaging characteristics:
- NECT: Isodense or hyper dense to brain or muscle
- MR: Hypo intense or Iso intense on T1-weighted MR images, heterogeneously Iso intense or hyper intense on T2-weighted MR images
- MR+C: Enhance homogeneously after injection of contrast medium
Paraspinal and intraspinal lesions are also thought to arise from perivenous arachnoid spread of leukemic cells. Uncommonly, spinal involvement by granulocytic sarcoma may cause compression of the spinal cord, cauda equina, or nerve roots