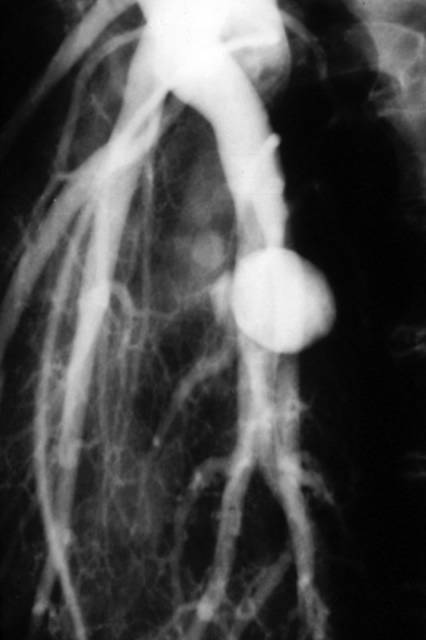
The "classical air-crescent sign"
Diagnosis- fungal ball or Aspergilloma!!!
COPYRIGHT (SUMER)

Tuberculosis risk high among Indian resident physicians
Resident doctors in India have nearly nine times the risk of contracting tuberculosis from their patients than the general population has of contracting the disease, researchers from Chandigarh, India, report.
"Due to the exceptionally high burden of tuberculosis in the general population in India, it is expected that doctors caring for such patients have a high probability of acquiring the disease," Dr. KG Rao and colleagues write.
To assess this increased risk, Dr. KG Rao and colleagues from the Post Graduate Institute of Medical Education and Research evaluated 873 doctors in various stages of their residencies.
The resulting study population was divided into two groups: group one - comprised of 470 doctors who were already undergoing residency in January 2001 when the study began, and group two, comprising 231 residents who joined during 2001. Researchers administered a detailed questionnaire on their medical history, previous and present exposure to tuberculosis, and treatment to group one at the start of the study and to group two after completion one year of training.
Thirteen residents in both groups, including nine (1.9%) in group one and 4 (1.7%) in group two contacted tuberculosis during the course of residency, giving an overall risk of 17.3 per 1000, nearly nine times higher than the population risk in India, Dr. Rao and colleagues report in the November issue of International Journal of Tuberculosis and Lung Diseases.
Extrapulmonary tuberculosis was predominant, with six (67%) residents in group 1 and three (75%) from group 2 developing this severe form of the disease, the researchers add. The incidence of extrapulmonary tuberculosis was significantly higher in the general population, probably because of repeated contact and prior exposure to tuberculosis, they suggest.
As compared to a previous 40-year cohort study on tuberculosis risk in US physicians, the risk of tuberculosis among Indian residents was eight times higher, the authors note. This could be due to the low tuberculosis prevalence in the US, they postulate.
"The most appropriate method of preventing such transmission is effective treatment of smear-positive pulmonary tuberculosis patients with standard four-drug anti-tuberculosis therapy, as most patients become non-infectious after 2 weeks of treatment if the organism is drug-sensitive," the authors conclude.
Int J Tuberc Lung Dis 2004; 8:1392-1394.
CT Appearance of Acute Appendagitis
OBJECTIVE: Our aim was to describe the spectrum of CT findings in patients with acute epiploic appendagitis and also to evaluate the changes seen with this condition.
MATERIALS AND METHODS: Fifty patients diagnosed with acute epiploic appendagitis seen on contrast-enhanced CT were included in this study. The CT scans of the epiploic appendagitis were evaluated for the presence of colon wall thickening, a focal fatty center, inflammatory changes, location in relationship to the colon, size, and presence or absence of central high density within the fat. In 10 patients, the initial findings were compared with findings of follow-up CT performed between 3 days-21 months after the first CT.
RESULTS: The most common part of colon involved by acute epiploic appendagitis was the sigmoid colon (31/50), and the most common position was anterior to the colonic lumen (41/50). All 50 patients with acute epiploic appendagitis had a central fatty core surrounded by inflammation. Colon wall thickening was present in only two, and a central high-density focus was noted only in 27 of 50 patients. In 86% (43/50) of patients, the fatty central core was between 1.5 and 3.5 cm in length. The changes seen on follow-up CT varied, including increased density with a decrease in the size of the fatty central core, no change, complete resolution of findings, and minimal residual density.
CONCLUSION: On CT, acute epiploic appendagitis has a predictable appearance in terms of location, size, and density. The most common finding on CT is a fat-density oval lesion with surrounding inflammation on the anterior aspect of the sigmoid colon. The changes on CT are not predictable in the 2-week to 6-month window.
AJR Am J Roentgenol. 2004 Nov;183(5):1303-7.