For those of you not aware of the whole story, this is Terri's Fight for life: The 15-year struggle
February 1990
Terri Schiavo collapses at home, the flow of oxygen to her brain is interrupted for five minutes, causing permanent damage.
1993
Michael Schiavo and wife's parents fall out over care she is receiving. The parents later try and fail to have Michael removed as Terri's guardian.
May 1998
Mr Schiavo files petition to remove feeding tube, but nothing is done until April 24 2001. Two days later medical evidence compels an appeal court to insist feeding begins again.
November 2002
A court agrees that Mrs Schiavo will not recover and orders her feeding tube to be removed again. This happens the following October. Florida governor Jeb Bush uses new legislation, Terri's Law, to demand that the tube be put back.
September 2004
Florida's supreme court rules Terri's Law unconstitutional. Appeal court sets March 18 2005 as day the tube will be removed.
March 18 2005
Judge orders the tube to be removed. Congress rushes through emergency bill which president signs - forcing a federal court to review decision.
March 22
Florida court stands by its judgment, so Mrs Schiavo's feeding tube will not be reconnected.
March 24
The US supreme court refuses another request to review the Schiavo case.
March 25
US district court turns down parents' request for an emergency order to force doctors to feed their daughter.Soon afterwards Florida supreme court turns down an emergency appeal.
March 30
Late Wednesday night, the US supreme court refuses for the sixth time to hear an appeal on Terri's plight.
March 31
Attorney David Gibbs announces that Terri Schiavo died at 9:05 Thursday morning (local time).
Terri Schiavo collapses at home, the flow of oxygen to her brain is interrupted for five minutes, causing permanent damage.
1993
Michael Schiavo and wife's parents fall out over care she is receiving. The parents later try and fail to have Michael removed as Terri's guardian.
May 1998
Mr Schiavo files petition to remove feeding tube, but nothing is done until April 24 2001. Two days later medical evidence compels an appeal court to insist feeding begins again.
November 2002
A court agrees that Mrs Schiavo will not recover and orders her feeding tube to be removed again. This happens the following October. Florida governor Jeb Bush uses new legislation, Terri's Law, to demand that the tube be put back.
September 2004
Florida's supreme court rules Terri's Law unconstitutional. Appeal court sets March 18 2005 as day the tube will be removed.
March 18 2005
Judge orders the tube to be removed. Congress rushes through emergency bill which president signs - forcing a federal court to review decision.
March 22
Florida court stands by its judgment, so Mrs Schiavo's feeding tube will not be reconnected.
March 24
The US supreme court refuses another request to review the Schiavo case.
March 25
US district court turns down parents' request for an emergency order to force doctors to feed their daughter.Soon afterwards Florida supreme court turns down an emergency appeal.
March 30
Late Wednesday night, the US supreme court refuses for the sixth time to hear an appeal on Terri's plight.
March 31
Attorney David Gibbs announces that Terri Schiavo died at 9:05 Thursday morning (local time).
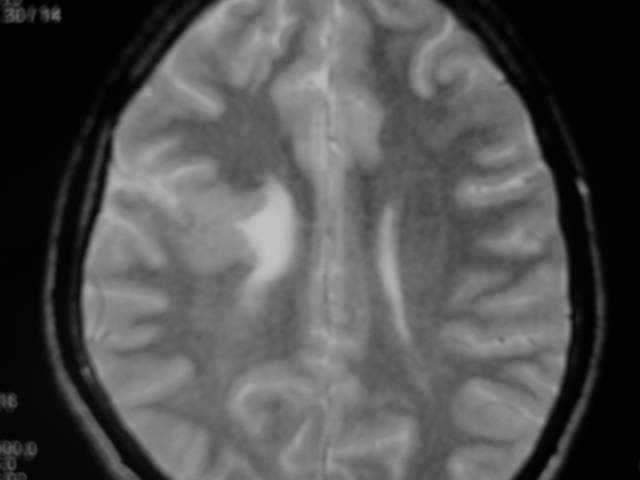
well for the interested people this is a single section of her CT scan available on the net, agreed there is cerebral atrophy but what is that white object in her lateral ventricle, is it a shunt put for hydrocephalus?? if it is a malfunctioning shunt would her prognosis be different?? any comments are welcome!

excellent discussion on this at-Codeblueblog



{kind=link}