Forbes Magazine has been ranking the 400 Richest Americans since way back in 1982. In that year's issue only 13 of the mighty 400 were billionaires, the rest had merely hundreds of millions of dollars.
Forbes Magazine has been ranking the 400 Richest Americans since way back in 1982. In that year's issue only 13 of the mighty 400 were billionaires, the rest had merely hundreds of millions of dollars.The 2006 issue came out last week. How many of the 400 are now worth a billion or more? The answer, after this....
Want to hear something interesting, well I think it's interesting....Flavor Flav has five children....their names are Shanique, 13; William Jr., 12; Karren, 11; Da'Zyna, 7; Quanah, 5; Kayla, 3.
Colleen, if we have a daughter....I want to name her Da'Zyna......please?

Jerry...you are wrong! Something interesting did happen in hockey this week.... The New York Islanders signed goalie Rick DiPietro to a 15-year contract where he will be making $4.75 million a year, for a total of $67.5 million! Talk about job security. His contract ends in 2021! He's going to be a 40-year old goalie...


Did you know that Rob Zombie got his start in show business as a production assistant on the Pee Wee's Playhouse?
Ok... Here's your answer....This year's Forbes 400 list of the richest Americans contains 400 billionaires for the first time! 999 million dollars doesn't even get you in the issue this year. Bill Gates is still number one with $53 billion....George Lucas was #70 with $3.6 billion, Steven Spielberg and Donald Trump were tied at #94 with $2.9 billion. Oprah is #235 with $1.4 billion....Martha Stewart dropped off the list this year. Poor poor Martha.










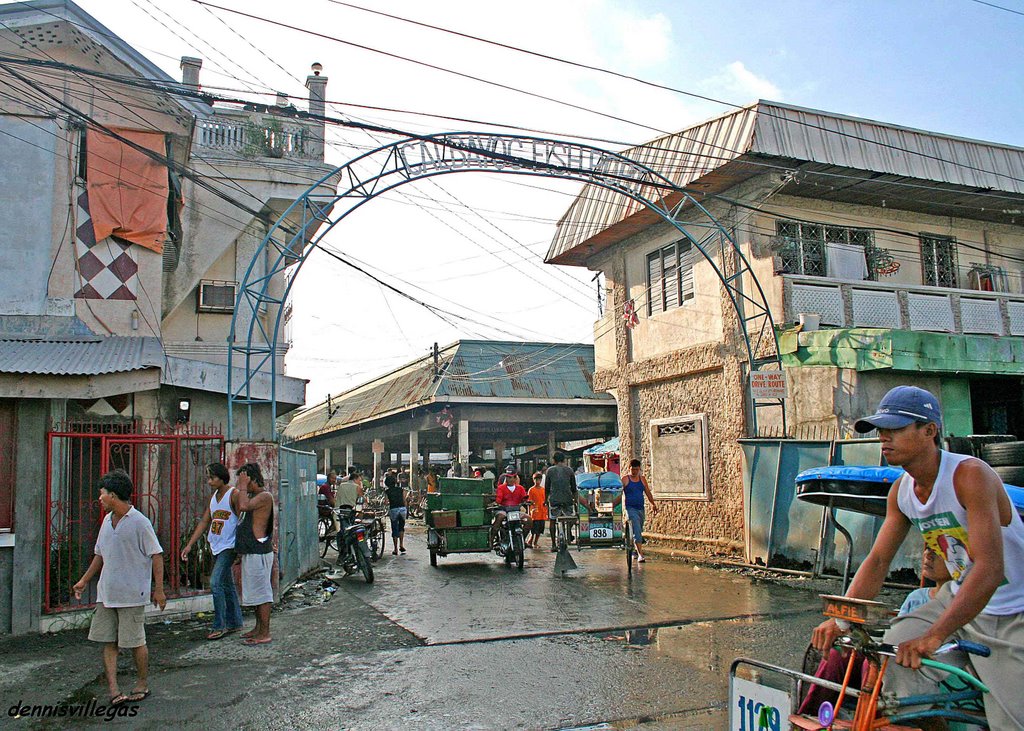


 Eduardo's Hotel, along Pajarito street. I stayed here during my first trip to Calbayog way back in 2004. This hotel is the best there is in Calbayog. They charge 700 pesos for a double-bed with aircondition, Cable TV, and hot and cold shower, with the benefit of ordering your food anytime day or night.
Eduardo's Hotel, along Pajarito street. I stayed here during my first trip to Calbayog way back in 2004. This hotel is the best there is in Calbayog. They charge 700 pesos for a double-bed with aircondition, Cable TV, and hot and cold shower, with the benefit of ordering your food anytime day or night.