There are days when I just feel lazy bringing along my beloved Nikon D80 during my walking tour, even though I want to shoot pictures everyday--just the kind of stuff I usually share with you: everyday sceneries, street people, nightscapes, and the like.
A few months ago, I sold my old reliable Sony DSC-T5, a camera which got me started in photography. Now I really regret having sold it, since I can still use that wonderful camera at times when a dslr is just too tiring to carry around, or is not allowed in a certain place-- like a mall, or a museum.
I really long for a digital compact camera that I can easily carry and not be as obtrusive as a big dslr. So, I decided to just purchase one anew. After all, I always thought that buying photographic equipments is a great investment.
Also, I always save some money because I don't have a vice that I must sustain- like smoking or drinking-and if photography is a vice, then it is a vice that can only be very rewarding, and not cause lung cancer and cirhossis of the liver.
After a little research on the internet, I decided to buy a Panasonic DMC-LX1 Lumix. It is a small digital compact, but it is big in features, like it has a Leica lens, an 8 megapixel sensor, and my favorite feature--an optical image stabilizer.
I read a lot of reviews before buying this camera. Generally, the reviews are great. It is an exceptional digital compact that delivers great images. But there has consistently been one bad issue with the DMC-LX1: Image noise when shooting dark or low light scenes.
I've just written in my previous entry that I love night photography. But then, night images can be easily taken cared of by my D80, so no problem with me about the image noise issue of the Lumix.
So, here then are some sample shots of my new digital compact, the Panasonic Lumix DMC-LX1. These photos are all straight out of the camera. No post-processing done except resizing. All are shot handheld using iso80.
You will notice that the photos are set at wide-angles because the Lumix has a unique parameter feature of 16:9, which appears as if you are viewing the photos from a wide cinema screen. Now isn't that cool!

Gen. Roxas St., Cubao
 The new Eurotel Hotel(or motel?) in Araneta Cubao
The new Eurotel Hotel(or motel?) in Araneta Cubao

Walkway to the cinema lobby of Gateway Mall where the Pacquiao-Morales III can be watched live. I had an account of the second fight in the January 2006 entry of my blog, where Pacquiao defeated Morales in the final round. This time around, though, Pacquaio simply demolished Morales in the third. I paid the 600 pesos ticket to watch it live. It was worth it.
 The cinema lobby of the new Gateway Mall. The domed ceiling remind me of the majestic domed ceiling of the ill-fated Titanic.
The cinema lobby of the new Gateway Mall. The domed ceiling remind me of the majestic domed ceiling of the ill-fated Titanic.

My favorite tambayan in the old Ali mall is of course National Bookstore. Syempre..laking National ako eh.

Fruit stand in the Farmers Market where I usually buy my favorite Durian, Lanzones, and Mangosteen fruits.
 The new Gateway Mall at dusk. Around 5 o'clock in the afternoon. As you can see, night time is now longer and daytime shorter.
The new Gateway Mall at dusk. Around 5 o'clock in the afternoon. As you can see, night time is now longer and daytime shorter.
 The giant Christmas Tree of Cubao..Ah..I'm very proud and fortunate to be a Cubao citizen!
The giant Christmas Tree of Cubao..Ah..I'm very proud and fortunate to be a Cubao citizen!
My personal assesment of the Panasonic Lumix DMC-LX1: I will not say much....I love this camera!







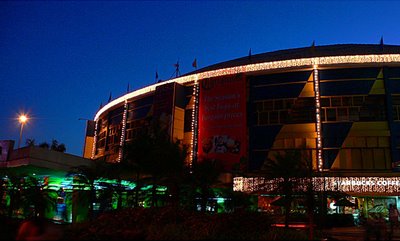 The Araneta Coliseum. Shot prior to my entry for the concert .
The Araneta Coliseum. Shot prior to my entry for the concert .

 The big LCD screen is a great benefit for those of us who cannot afford the ringside seats.
The big LCD screen is a great benefit for those of us who cannot afford the ringside seats. The audience are dancing and clapping, to the tune of "Tragedy",
The audience are dancing and clapping, to the tune of "Tragedy", The encore..Robin Gibb delighted his fans with two encores!
The encore..Robin Gibb delighted his fans with two encores!


 The crowd excitedly awaiting Robin Gibb
The crowd excitedly awaiting Robin Gibb Robin singing my favorite song "First of May".
Robin singing my favorite song "First of May". The audience danced to its feet as Robin sang the hugely popular
The audience danced to its feet as Robin sang the hugely popular Waving goodbye to his fans, promising that next time, he'd bring along his brother Barry.
Waving goodbye to his fans, promising that next time, he'd bring along his brother Barry. The crowd outside the Araneta Coliseum, right after the concert.
The crowd outside the Araneta Coliseum, right after the concert.


 The new Eurotel Hotel(or motel?) in Araneta Cubao
The new Eurotel Hotel(or motel?) in Araneta Cubao
 The cinema lobby of the new Gateway Mall. The domed ceiling remind me of the majestic domed ceiling of the ill-fated Titanic.
The cinema lobby of the new Gateway Mall. The domed ceiling remind me of the majestic domed ceiling of the ill-fated Titanic.

 The new Gateway Mall at dusk. Around 5 o'clock in the afternoon. As you can see, night time is now longer and daytime shorter.
The new Gateway Mall at dusk. Around 5 o'clock in the afternoon. As you can see, night time is now longer and daytime shorter. The giant Christmas Tree of Cubao..Ah..I'm very proud and fortunate to be a Cubao citizen!
The giant Christmas Tree of Cubao..Ah..I'm very proud and fortunate to be a Cubao citizen! Dusk at Edsa Cubao. Shot from the Cubao Overpass. I placed my Nikon on the railing of the camera so I was able to make a 2 second exposure.
Dusk at Edsa Cubao. Shot from the Cubao Overpass. I placed my Nikon on the railing of the camera so I was able to make a 2 second exposure. The colored trees of Cubao
The colored trees of Cubao Shopwise Supermarket
Shopwise Supermarket


 The new Gateway Mall
The new Gateway Mall A busy street in Cubao
A busy street in Cubao













