HAPPY NEW YEAR 2005 TO ALL!!!
COPYRIGHT (SUMER)
And the old lady cries.
And the lonely children suffer.
Their mother's now alone.
Their fathers wont come home.
And the old lady cries.
And the old lady cries.
The gods were hungry.
And the gods weren't happy.
They had offered their jewellery
They had paid and prayed only.
But the stones know no mercy.
Their hunger must be appeased.
While the guilty run free.
The innocent are punished.
But the little girl asks.
Why were we punished?
What did we do wrong?
We would have followed
Had we been told
And the old lady cries.
Her son will not return.
Her faith will not rise
The stones, she will burn.And the anger wont subside.
Like the waves killed her love.
Her revenge will come.
Her children she must save.
But her anger wont subside.
Darker-Side-Of-Saturn
USGS: Warnings Could Have Saved Thousands in Asia
A warning center such as those used around the Pacific could have saved most of the thousands of people who died in Asia's earthquake and tsunamis, a U.S. Geological Survey official said on Sunday.
None of the countries most severely affected -- including India, Thailand, Indonesia and Sri Lanka -- had a tsunami warning mechanism or tidal gauges to alert people to the wall of water that followed a massive earthquake, said Waverly Person of the USGS National Earthquake Information Center.
"Most of those people could have been saved if they had had a tsunami warning system in place or tide gauges," he said.
"And I think this will be a lesson to them," he said, referring to the governments of the devastated countries.
Person also said that because large tsunamis, or seismic sea waves, are extremely rare in the Indian Ocean, people were never taught to flee inland after they felt the tremors of an earthquake.
Tsunami warning systems and tide gauges exist around the Pacific Ocean, for the Pacific Rim as well as South America. The United States has such warning centers in Hawaii and Alaska operated by the U.S. Geological Survey. But none of these monitors the Indian Ocean region.
The 8.9-magnitude underwater quake -- one of the most powerful in history -- off the Indonesian island of Sumatra devastated southern Asia and triggered waves of up to 30 feet high.
U.S. seismologists said it was unlikely the Indian Ocean region would be hit any time soon by a similarly devastating tsunami because it takes an enormously strong earthquake to generate one.
"That's really what has created all of these problems -- is that the earthquake is just so massive," said Dan Blakeman, a USGS earthquake analyst.
But Person said governments should instruct people living along the coast to move after a quake. Since a tsunami is generated at the source of an underwater earthquake, there is usually time -- from 20 minutes to two hours -- to get people away as it builds in the ocean
FROM-WASHINGTON (Reuters)
Effects of repeated prenatal ultrasound examinations on childhood outcome up to 8 years of age: follow-up of a randomised controlled trial.
Newnham JP, Doherty DA, Kendall GE, Zubrick SR, Landau LL, Stanley FJ
BACKGROUND: Despite the widespread use of prenatal ultrasound studies, there are no published data from randomised controlled trials describing childhood outcomes that might be influenced by repeated ultrasound exposures. We previously undertook a randomised controlled trial to assess the effects of multiple studies on pregnancy and childhood outcomes and reported that those pregnancies allocated to receive multiple examinations had an unexplained and significant increase in the proportion of growth restricted newborns. Our aim was to investigate the possible effects of multiple prenatal ultrasound scans on growth and development in childhood. Here, we provide follow-up data of the childrens' development. METHODS: Physical and developmental assessments were done on children whose pregnant mothers had been allocated at random to a protocol of five studies of ultrasound imaging and umbilical artery Doppler flow velocity waveform between 18 and 38 weeks' gestation (intensive group n=1490) or a single imaging study at 18 weeks' gestation (regular group n=1477). We used generalised logistic and linear regression models to assess the group differences in developmental and growth outcomes over time. Primary data analysis was done by intention-to-treat. FINDINGS: Examinations were done at 1, 2, 3, 5, and 8 years of age on children born without congenital abnormalities and from singleton pregnancies (intensive group n=1362, regular group n=1352). The follow-up rate at 1 year was 85% (2310/2714) and at 8 years was 75% (2042/2714). By 1 year of age and thereafter, physical sizes were similar in the two groups. There were no significant differences indicating deleterious effects of multiple ultrasound studies at any age as measured by standard tests of childhood speech, language, behaviour, and neurological development. INTERPRETATION: Exposure to multiple prenatal ultrasound examinations from 18 weeks' gestation onwards might be associated with a small effect on fetal growth but is followed in childhood by growth and measures of developmental outcome similar to those in children who had received a single prenatal scan.
Lancet. 2004 Dec 4;364(9450):2038-44

Tuberculosis risk high among Indian resident physicians
Resident doctors in India have nearly nine times the risk of contracting tuberculosis from their patients than the general population has of contracting the disease, researchers from Chandigarh, India, report.
"Due to the exceptionally high burden of tuberculosis in the general population in India, it is expected that doctors caring for such patients have a high probability of acquiring the disease," Dr. KG Rao and colleagues write.
To assess this increased risk, Dr. KG Rao and colleagues from the Post Graduate Institute of Medical Education and Research evaluated 873 doctors in various stages of their residencies.
The resulting study population was divided into two groups: group one - comprised of 470 doctors who were already undergoing residency in January 2001 when the study began, and group two, comprising 231 residents who joined during 2001. Researchers administered a detailed questionnaire on their medical history, previous and present exposure to tuberculosis, and treatment to group one at the start of the study and to group two after completion one year of training.
Thirteen residents in both groups, including nine (1.9%) in group one and 4 (1.7%) in group two contacted tuberculosis during the course of residency, giving an overall risk of 17.3 per 1000, nearly nine times higher than the population risk in India, Dr. Rao and colleagues report in the November issue of International Journal of Tuberculosis and Lung Diseases.
Extrapulmonary tuberculosis was predominant, with six (67%) residents in group 1 and three (75%) from group 2 developing this severe form of the disease, the researchers add. The incidence of extrapulmonary tuberculosis was significantly higher in the general population, probably because of repeated contact and prior exposure to tuberculosis, they suggest.
As compared to a previous 40-year cohort study on tuberculosis risk in US physicians, the risk of tuberculosis among Indian residents was eight times higher, the authors note. This could be due to the low tuberculosis prevalence in the US, they postulate.
"The most appropriate method of preventing such transmission is effective treatment of smear-positive pulmonary tuberculosis patients with standard four-drug anti-tuberculosis therapy, as most patients become non-infectious after 2 weeks of treatment if the organism is drug-sensitive," the authors conclude.
Int J Tuberc Lung Dis 2004; 8:1392-1394.
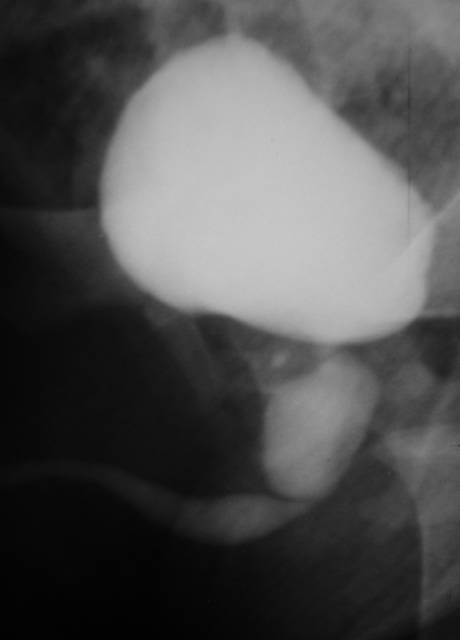
CT Appearance of Acute Appendagitis
OBJECTIVE: Our aim was to describe the spectrum of CT findings in patients with acute epiploic appendagitis and also to evaluate the changes seen with this condition.
MATERIALS AND METHODS: Fifty patients diagnosed with acute epiploic appendagitis seen on contrast-enhanced CT were included in this study. The CT scans of the epiploic appendagitis were evaluated for the presence of colon wall thickening, a focal fatty center, inflammatory changes, location in relationship to the colon, size, and presence or absence of central high density within the fat. In 10 patients, the initial findings were compared with findings of follow-up CT performed between 3 days-21 months after the first CT.
RESULTS: The most common part of colon involved by acute epiploic appendagitis was the sigmoid colon (31/50), and the most common position was anterior to the colonic lumen (41/50). All 50 patients with acute epiploic appendagitis had a central fatty core surrounded by inflammation. Colon wall thickening was present in only two, and a central high-density focus was noted only in 27 of 50 patients. In 86% (43/50) of patients, the fatty central core was between 1.5 and 3.5 cm in length. The changes seen on follow-up CT varied, including increased density with a decrease in the size of the fatty central core, no change, complete resolution of findings, and minimal residual density.
CONCLUSION: On CT, acute epiploic appendagitis has a predictable appearance in terms of location, size, and density. The most common finding on CT is a fat-density oval lesion with surrounding inflammation on the anterior aspect of the sigmoid colon. The changes on CT are not predictable in the 2-week to 6-month window.
AJR Am J Roentgenol. 2004 Nov;183(5):1303-7.


NEW NEW NEW...... NOW AVAILABLE
All India PG entrance exam 2005 fully solved by Dr Sumer K Sethi and Dr Sidharth K Sethi is now available in the market!!!
this is only authentic solution to aipg 2005 available till now, it has explanatory answer from latest editions of standard textbooks with extensive online support at www.sumerdoc.blogspot.com
AIIMS NOV 2004 FULLY SOLVED AND EXPLAINED
aiims nov 2004 fully solved and explained by sumer sethi is availlable in the market...highlights of the book are authentic references, diagrams and flowcharts, extensive coverage of topics so that all repeat questions are tackled...and first book of its kind to give extensive online support with an online discussion forum support by the author.. also by the same author "review of radiology" solving quite a few questions in this aiims!! and may 2004 aiims fully solved peepee publishers
to order any book of peepee publishers for pg entrance preparation- including AIPG JAN 2005(Rs165/-), NOV 2004 AIIMS (Rs150/-),MAY 2004 AIIMS (Rs 95/-) solved by me and Review Of Radiology (Rs100/-) a must for all PG aspirants for radiology
simply fill in ur details including name, email address and phone number and mailing address.. write or mail to
and address-
Peepee publishers and distributors (P) ltd
7/31 ansari road, darya ganj,
post box no-7243
new delhi 110002
india
SEND A CHEQUE/ D/D TO THE ABOVE ADDRESS
SPECIAL OFFER-NO POSTAGE WUD BE REQUIRED FOR ORDERS IN INDIA
----------------------------------------------------------------------------------------------------------
ALSO ON--
MY BOOKS AVAILABLE ONLINE-- NO BOOK SHOPS REQUIRED
my book "review of radiology" if it is not available in your city or if u ve any problem purchasing the book check out the link-
http://www.mcqsonline.com/edoctor/radiology_review.htm
also if u want MAY 2004 solved paper by sumer sethi extensively researched solutions to may 2004 aiims click here--
http://www.mcqsonline.com/edoctor/aiims_2004.htm
also available at
http://www.geocities.com/grajesh70/bookstore.htm
FOR NOV AIIMS TO ORDER ONLINE--
http://www.edoctor.mcqsonline.com/aiims_nov_2004.htm
TO ORDER ASHWIN UDAYAR'S MAHE GUIDE WITH 2000-2004 PAPERS
www.mcqsonline.com/edoctor/mahe_2004.htm