



















 This is Avenida, one of the busiest boulevards in Manila. Here you will find all kinds of people, bartering, selling, or buying, or just strolling around looking for someone to love :P. I always walk along Avenida after my work, and not a few times was I approached by a girl or an older lady offering their bodies for a few hundred pesos. If you have a keen eye you can spot some of them in this picture.
This is Avenida, one of the busiest boulevards in Manila. Here you will find all kinds of people, bartering, selling, or buying, or just strolling around looking for someone to love :P. I always walk along Avenida after my work, and not a few times was I approached by a girl or an older lady offering their bodies for a few hundred pesos. If you have a keen eye you can spot some of them in this picture. This is Plaza Lacson in Sta. Cruz. This photo was taken from the LRT Carriedo Station in Sta. Cruz. The Old Prudential Bank Building is in the background. In front of it is the perrenial statue of Mayor Arsenio Lacson.
This is Plaza Lacson in Sta. Cruz. This photo was taken from the LRT Carriedo Station in Sta. Cruz. The Old Prudential Bank Building is in the background. In front of it is the perrenial statue of Mayor Arsenio Lacson.

 This is the regular menu in Ma Mon Luk. The food may be a little more expensive than McDonalds or Jolibee, but I tell you I will never trade Ma Mon Luk Siopao with the Big Mac. I really like that byline "Ang Mami dito ay unang imbento, Una sa Lasa, Una sa Sarap". Now that is really cool, doesn't it?
This is the regular menu in Ma Mon Luk. The food may be a little more expensive than McDonalds or Jolibee, but I tell you I will never trade Ma Mon Luk Siopao with the Big Mac. I really like that byline "Ang Mami dito ay unang imbento, Una sa Lasa, Una sa Sarap". Now that is really cool, doesn't it?
Ever since I had my Rebel XT, I just miss my little compact Sony DSC-T5. So I took it out of my pocket and exercised its legs.
It still takes good pictures despite its being 2 years old(an octogenarian for a camera).
And here are some of them:
Well, these guys are the waiters of Ma Mon Luk. All of them are regulars there, and some have been waitering there even when Ma Mon Luk was still living. They may be snobbish the first you meet them, but I tell you if you eat there, kindly leave 10 or 20 pesos in tip and the next time you eat there, they'll treat you like a king!
I'll post more pictures soon. Meanwhile it's time to take some rest...in the restroom.




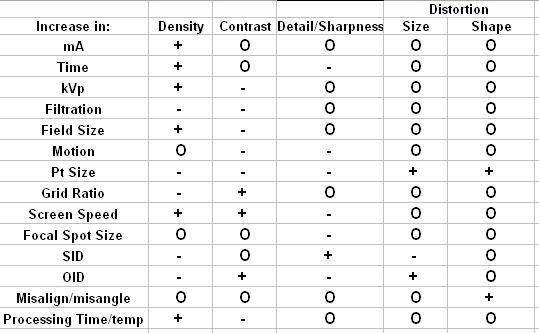 + = increase, - = decrease, O = no change
+ = increase, - = decrease, O = no change











{kind=link}
{kind=link}
{kind=link}